
Many patients wonder why Eyes Alive work the way we do.
Surely an Ocular Prosthesis can be made in less time.
In the old days, eyes were made in a day.
Over the last few years, one of the biggest concerns in the manufacturing of an Ocular Prosthetic is Free Monomer in ocular prosthetics after curing the prosthesis.
Globally, lots of research and debate exists around this matter.
In essence, there is agreement that the old philosophy of short single-stage curing is no longer appropriate.
When a prosthesis is cured too quickly, it potentially leaves free monomer trapped inside the prosthesis.
With Free monomer in the prosthesis, the patient will often experience symptoms like dry-eye, excessive discharge, and overall discomfort.
Some patients interpret this discharge as an infection in the socket and visit their local GP or Ophthalmologist for antibiotic treatment. The symptoms often clear up and repeat soon after the prescribed medication course ends. This confirmed the problem is more likely related to the prosthesis than the socket, and the patient should visit their Ocularist.
At Eyes Alive, we made the decision that our patient's wellbeing is paramount, and therefore we manufacture our eyes without exception using a slower multistage process, which is in line with globally accepted best practices. Although this takes much longer to manufacture and fit an eye, and costs Eyes alive a lot more resources, the patients overall report a happier experience wearing their prosthesis.
A quick look at why practitioners should be worried about free monomer or residual monomer in the prosthesis.
https://en.wikipedia.org/wiki/Methyl_methacrylate
Wikipedia defines the molecule as follows:
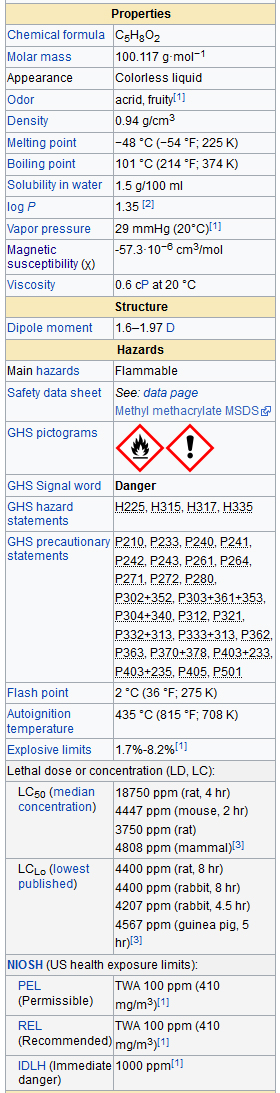
A quick visit to Wikipedia and the toxic value of monomer is evident.
In rat studies, where rats are exposed to the vapours of Monomer, death occurs in less than two hours.
Monomer’s flashpoint or, the temperature that it evaporates varies between sources, but it is generally accepted to be between 2o C and 12o C.
This, in turn, means any monomer trapped in the prosthesis will leach out into the socket for the life of the prosthesis, due to the body being at a constant 37o C.
(Note that most of the literature indicates that the critical period is the first 48 hours from manufacturing, after which the residual levels seem to drop and are quite low. However, low these levels may be, there remain associated health hazards).
The eye socket is similar to the mouth, where the same dental materials are used, in the sense that it has wet tissue.
Wet tissue assists the monomer to leach, and the free monomer in the body fluids is then easily absorbed into the blood stream and circulated through the body.
Studies indicate that the first 24-48 hours is most significant.
Therefore, if we extend our curing process to include an additional 24-hours, we can almost guarantee the best result for our patients, with the lowest possible monomer dosing.
Multistage curing
What is multistage curing?
The old philosophy was to place the acrylic into water and heat it immediately in one step to 100 degrees. This for reasons explained below is not ideal, so the curing unit needs to be able to raise the temperature in a controlled fashion, in steps or ramps, i.e. take the water with the prosthesis up to a lower temp, say 53 degrees, over a predetermined timeframe, of say 15 minutes, then hold at that temp for some time before it raised again to a higher temperature. This allows the temperature to penetrate the full thickness of the mould which houses the prosthesis during the curing.
Although the acrylic manufacturer specifications, in some instances, only call for a 15-minute cure at 100 degrees. This specification is designed to achieve the maximum material strength of the acrylic; however, there is enough documented scientific evidence to show this is not good enough for patients as it may not remove the free monomer.
Another concern of some researchers is that when you place a sample of material into a curing vessel and take it straight to 100 degrees, you get what is referred to as case hardening or shell hardening.
What this means is that if your curing vessel is switched on and allowed to heat up at the maximum rate of the element, the outside of the prosthesis heats up much faster than the inside section, thus as the outside of the prosthesis cures, and it traps some of the monomer in the prosthesis before the inner part reaches the temp required to cure.
At Eyes Alive, our curing programme, the first stage will be taking the water from ambient temp or room temp to 53o C, and we programme this to take 15 minutes.
By forcing the element to work slower, we guarantee that the entire prosthesis cures at a uniform temperature throughout. This, in turn, minimises the possibility of Shell Hardening and trapping monomer within the prosthesis.
The controller then holds the temp at 53o C for a time before starting the next ramp which eventually takes our temp up to 97o C.
This process is referred to in the thermal industry as Ramp Control.
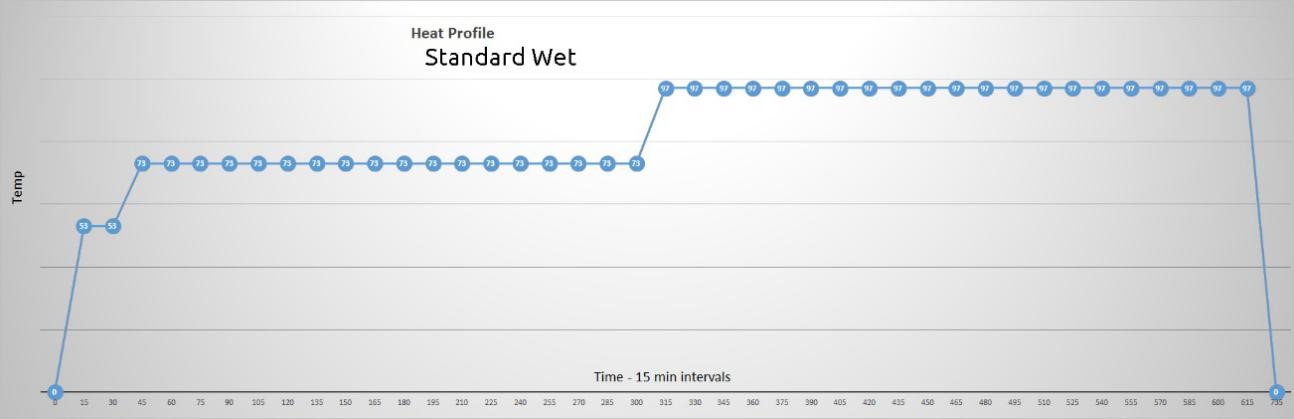
Below, I will describe the full heat profile we use to cure eyes at Eyes Alive.
Our heat profile has been developed and tweaked over a number of years, taking cognisance of global best practices.
This curing process must happen for each stage of the eye, so you can understand that most curing is done overnight, and the eye gets cured between each appointment with the patient, which means the cumulative time to make an eye is a minimum of three days.
The GRAND PRIZE, is we don’t have patients with sensitivity to monomer.
We have, however, had several patients where their prosthesis was made elsewhere, and they have approached us with a complaint of irritations to the socket.
In most cases, if we can run their prosthesis through our multistage curing process, and these symptoms are a thing of the past.
Establishing a good ramp profile/heat profile for curing an eye.
In our practice, the heat profile or ramp profile we use has been developed to what we believe gives the patient maximum security that they will not likely experience any socket irritations from the residual monomer.
Our programme looks like this:
Ramp 1 - Ambient to 53o C over 15 minutes
Ramp 2 - Hold at 53o C for 15 minutes
Ramp 3 - 53o C to 73o C over 15 minutes
Ramp 4 - Hold at 73o C for 4 hours
Ramp 5 - 73o C to 97o C over 15 minutes
Ramp 6 - hold at 97o C for 5 hours
Ramp 7 - 97o C back to ambient temp in its own time
This reiterates why manufacturing an eye in a day does not happen in our practice.
In fact, curing each stage in this manner forces manufacturing to take, at the very least, three days per patient, excluding the variance, of needing to make adjustments and where necessary allow the patient to reduce swelling, wear the model to Confirm comfort over a few days or other unforeseen inconveniences.
From the above explanation, we can be guaranteed that we have reached maximum tensile strength, and the acrylic will be stable and well within the manufacturer's specifications.
However, we can’t be sure of what free monomer is left in the prosthesis in the form of the residual monomer or free monomer that can leach out over the rest of the prosthesis’ lifespan.
So, looking at the literature on best practices to remove free monomer.
It is suggested to let the final prosthetic eye soak for a further 24 hours in distilled water at 53o C.
Ideally one must use distilled water, as there will be zero dissolved solids and other contaminants in the water, which will allow maximum leaching.
Thereafter, the prosthesis is polished to a high gloss and fitted to the patient.
All this work enforces Eyes Alive’s commitment to service excellence and customer satisfaction.

Download this document to learn more about Free Monomer.
Resources
- OASA PROVIDER QUALITY ASSURANCE POLICY DOCUMENT
OASA Policy 007 This policy adopted by members of OASA On the 16 day of November 2010
President: PI Carvalho Amended on the 16 day of October 2016 - COMPARATIVE EVALUATION ON THE INFLUENCE OF DIFFERENT CURING CYCLES ON THE MECHANICAL PROPERTIES OF THREE COMMERCIALLY AVAILABLE DENTURE BASE RESINS: AN IN-VITRO STUDY
Journal of Applied Dental and Medical Sciences NLM ID: 101671413 ISSN:2454-2288 Volume 2 Issue3 July- September 2016 - The Traditional and a Two-cycle Method
Gefei Wang
The Ohio State University - Cytotoxicity of Acrylic Resin: A Review
Arunasree V Mallikarjuna
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861. Volume 13, Issue 3 Ver. II. (Mar. 2014), PP 07-09 www.iosrjournals.org www.iosrjournals.org 7 | Page - Mass Spectrometry of Polymers
Giorgio Montaudo and Robert P. Lattimer, Eds.
ISBN 0-8493-3127-7 - Detection and quantification of monomers in unstimulated whole
2Dental University Hospital,University of Bergen, Bergen; 3Nordic Instituteof Dental Materials (NIOM), Oslo; 4Dental Biomaterials Adverse Reaction Unit, Uni - Effect of leaching residual methyl methacrylate concentrations on in vitro Cytotoxicity of heat polymerized denture base acrylic resin processed with different polymerization cycles
Canan BURAL12, Gunnur DENIZ3 4, Gulsen BAYRAKTAR5 Faculty of Dentistry - Department of Removable Prosthodontics - Capa, 34390 - Istanbul - Turkey - FACTORS INFLUENCING SORPTION, SOLUBILITY AND CYTOTOXICITY OF A HEAT CURED DENTURE BASE POLYMER
Magdalena Aletta Engelbrecht Faculty of Dentistry University of the Western Cape
November, 2010. - Laboratory Evaluation of Newly Formulated Thermoplastic Resin Complete Denture Base Materials
El-Khodary N. M.1, , Alexandria University, Egypt - Mass Spectrometry of Polymers and Polymer Surfaces
S. D. Hanton Allentown, Pennsylvania 18195 Received April 4, 2000 - Research Journal of Pharmaceutical, Biological and Chemical Sciences
Cytotoxicity of denture base resins and preventive measures.
Nandhini Ashok1*, Dhanraj Ganapathy2
1Intern, Department Of Prosthodontics, Saveetha Dental College, Chennai, Tamil Nadu, India.
2Professor & HOD, Department Of Prosthodontics, Saveetha Dental College, Chennai, Tamil Nadu, India.
March – April 2017 RJPBCS 8(2) Page No. 155 - Comparative effect of different polymerization techniques on residual monomer and hardness properties of PMMA-based denture resins
Elif Aydogan Ayaz1, Rukiye Durkan2, Ays¸egul Koroglu3, Bora Bagis4
1 Department of Prosthodontics, Faculty of Dentistry, Karadeniz Technical University, Trabzon – Turkey - Effects of water boiling, microwave, and water bath post-polymerization on mechanical properties of acrylic denture resins
Milena Kostić1, Ljubisa Nikolic2, Vesna Nikolic2, Dušan Petković3, Marko Igić1, Nebojša Krunić1, Miodrag Manić3, Nikola Gligorijević1, Goran Radenković3
1University of Niš, Medical Faculty, Bulevar dr Zorana Đinđića 81, Niš, Serbia 2University of Niš, Faculty of Technology, Bulevar Oslobođenja 124, Leskovac, Serbia 3University of Niš, Faculty of Mechanical Engineering, Aleksandra Medvedeva 14, Niš, Serbia - Effect of processing and curing procedures on residual monomer levels of denture base materials
Amornrat Wonglamsam1, Wanicha Kaewkornpradit2, Noppavan Nagaviroj1, Widchaya Kanchanavasita1
Department of Prosthodontics, Faculty of Dentistry, Mahidol University - Research Article Effect of Pressure, Post-Pressing Time, and Polymerization Cycle on the Degree of Conversion of Thermoactivated Acrylic Resin
Rafaella de S. Leão ,1 Sandra L. D. de Moraes,2K´atia A.da S.Aquino ,3 Cristina P. Isolan,4Bruno G. da S. Casado ,1 and Marcos A. J. R. Montes1
1Department of Restorative Dentistry, Faculty of Dentistry, University of Pernambuco-FOP/UPE, - Polymerization cycles on hardness and surface gloss of denture bases
Rafael Leonardo Xediek Consani, Maria Giulia R. Pucciarelli, Marcelo F. Mesquita, Moises C. F. Nogueira,
Valentim A. R. Barão
Department of Prosthodontics and Periodontology, Piracicba Dental School, State University of Campinas, Piracicaba, SP, Brazil - Određivanje količine rezidualnog monomera u pojedinim akrilatima za bazu proteze i mogućnosti njegove redukcije
Milena Kostić*, Nebojša Krunić†, Ljubiša Nikolić‡, Vesna Nikolić‡,Stevo Najman§, Jelena Kocić§Klinika za stomatologiju, *Odeljenje za stomatološku protetiku, Niš; Medicinski fakultet Niš, †Odsek stomatologija, §Institut za biomedicinska istraživanja, Niš; Tehnološki fakultet Leskovac, Leskovac, Srbija - THE RESIDUAL MONOMER IN DENTAL ACRYLIC RESIN AND ITS ADVERSE EFFECTS
Nedeljka Ivković1,*, Djordje Božović1, Siniša Ristić1, Vladan Mirjanić2, Olivera Janković2
Faculty of Medicine, Department of stomatology, University of East Sarajevo, Republic of Srpska - Vertex SAFETY DATA SHEET SDS ID: M--MOA-2015-04-UK
SECTION 1: IDENTIFICATION OF THE SUBSTANCE/MIXTURE AND THE COMPANY/UNDERTAKING
Product identifier Product name Vertex Monomer Type A Product description Monomer based on Methyl Methacrylate
Alternative names Vertex Rapid Simplified, Vertex Regular, Vertex Implacryl, Vertex Implacryl Cold, Vertex Castapress, Vertex Castavaria, Vertex TCA,Vertex Teeth Material, Vertex BasiQ 20, Platinum HI, J-Cryl+.
SDS ID.:MMOA201504UK Page 1 of 9 (Date: 12/15) - The low-allergen denture
J.M. Kreijns, MA, is a dentistry consultant and practising dent dentist.
He was editor of TandartsPraktijk between 1990 and 2010. - Allergic effects of the residual monomer used in denture base acrylic resins
Haroon Rashid, Zeeshan Sheikh, and Fahim Vohra
Department of Prosthodontics, College of Dentistry, Ziauddin University, Karachi, Pakistan - Residual Monomer of Autopolymerized Acrylic Resin According to Different Manipulation and Polishing Methods
Tatiana Siqueira Gonc¸alvesa; Luciane Macedo de Menezesb;Luiz Ernani Aguiar Silvac
Angle Orthodontist, Vol 78, No 4, 2008 - Effect ofmethylmethacrylatemonomeronbondstrengthofdenturebase resintoacrylicteeth
Julieˆ Marra a, Andre´ GustavoPaleari a, AnaCarolinaPero a, RaphaelFreitasdeSouza b, De´boraBarrosBarbosa c, MarcoAntonioCompagnoni a, _ a Department Dental Materials and Prosthodontics, Araraquara dental school, Sao Paulo StateUniversity, UNESP, RuaHumaita´, Article history: Accepted30June2008 Availableonline15August2008 - Why You Should Be Cautious Of Getting Acrylic Nails
By Dana Oliver, 02/22/2016 04:31 pm ET | Updated February 23, 2016, /On HuffPost - The hidden dangers of acrylic nails and why you might want to re-think getting them
Alexandra Brown, AOL.com Oct 22nd 2015 2:21 PM
Contact Us
Operating Hours
Monday - Friday: 9:30 am - 5:00 pm
1 Saturday a month: By appointment only
Sunday: Closed
Let us call you
Provide your details to us and we will be in touch with you.